May serves as Hypermobility Spectrum Disorder (HSD) and Ehlers-Danlos Syndromes (EDS) Awareness Month. Additionally and aptly May also represents Mental Health Awareness Month. Those of us with lived experience trying to manage these conditions and navigate healthcare systems can appreciate the two go hand-in-hand. The goal of HSD & EDS Month is to raise awareness, improve diagnostic timelines, expand treatment options, and to fund research opportunities towards such. Much has been learned since the initial proclamation 10 years ago and emphasis continues to be placed on exploring the impact of HSD and EDS on body-wide systems as well as impacts on symptom management from integrative medicine modalities.
Introduction to Hypermobility Spectrum Disorder (HSD)
Hypermobility can simply refer to being flexible, “double-jointed”, or allude to a joint moving beyond the normal range of motion. It becomes a disorder when there is pain, instability, sprains, partial or full dislocations that may negatively impact one’s livelihood and functioning. Each person can experience a variety of symptoms with differing degrees of severity, hence naming it a “spectrum” disorder, although this is not in a traditional linear sense. Hypermobility Spectrum Disorder (HSD) includes four types-general, peripheral, localized, and historical.
- Generalized-Joint hypermobility occurs throughout the body.
- Peripheral-Joint hypermobility specific to hands and feet.
- Localized-Hypermobility in one particular joint or multiple joints in a specific region.
- Historical-Past exams are positive for generalized hypermobility but there is no current evidence of such.
Introduction to Hypermobile Ehlers-Danlos Syndrome (hEDS)
Ehlers-Danlos Syndrome (EDS) is an inheritable disorder which primarily impacts the production, processing, and structure of collagen (an integral component of connective tissues). There are 14 subtypes of EDS, the most common of which is hEDS. Much like HSD, hEDS is a multi-system disorder with a spectrum of signs, symptoms, and severities. In this way, emphasis is placed on individualizing treatment and management. Typically, the skin is impacted more so than HSD, with increased skin laxity, soft/velvety texture, presence of papules, fragility, and elasticity. HSD and hEDS have many overlapping signs and symptoms as well.
| Subtypes of Ehler-Danlos Syndrome | Significant Traits |
|---|---|
| Arthrochalasia EDS (aEDS) | Congenital, bilateral hip dislocation, hypermobility |
| Brittle Cornea Syndrome (BCS) | Cornea fragility, hearing loss, blue sclerae, hypermobility |
| Cardiac-Valvular EDS (cvEDS) | Severe heart valve problems, hypermobility |
| Classical EDS (cEDS) | Stretchy skin, easy bruising, hernias, prolapse, hypermobility |
| Classical-Like EDS (clEDS) | Soft stretchy skin, easy bruising, hypermobility |
| Dermatosparaxis EDS (dEDS) | Excess skin, skin fragility, facial changes, easy bruising, hypermobility, short limbs, hernia, soft doughy skin |
| Hypermobile EDS (hEDS) | Chronic pain, hypermobility |
| Kyphoscoliotic EDS (kEDS) | Low muscle tone, kyphoscoliosis, hypermobility, arterial dissection / rupture, eye problems, hearing loss |
| Musculocontractural EDS (mcEDS) | Congenital joint contractures, skeletal abnormalities, hypermobility, hypotonia, long fingers |
| Myopathic EDS (mEDS) | Joint contractures, delayed motor development, muscle weakness |
| Periodontal EDS (pEDS) | Severe early onset periodontitis, premature loss of teeth, pretibial plaques, hypermobility, skin fragility |
| Spondylodysplastic EDS (spEDS) | Bone growth changes, joint contractures & hypermobility, short stature, low muscle tone |
| Vascular EDS (vEDS) | Fragile connective tissue, aneurysms, dissection, ruptures of arteries and organs, absent earlobes, fistulas, perforations |
| Classical-Like Type 2 EDS (clEDS2) | Severe joint & skin laxity, ruptures, prolapse, skeletal abnormalities, osteoporosis, osteoarthritis |
Diagnosing HSD and hEDS
Not all practitioners may formally diagnose hEDS or HSD, although a diagnosis is not necessary to treat symptoms of such. Instead, they may recognize clinical presentations, perform screenings, help manage symptoms, and refer to specialists like Rheumatologists, Physiatrists, and Geneticists.
Genetic testing may be done to confirm particular subtypes of EDS in addition to the 200+ other connective tissue disorders. However, there are no current genetic tests available for confirming hEDS or HSD specifically.
Your provider will want to discuss medical history, family health history, and any current symptoms you may be experiencing. Additionally, they’ll perform a physical exam typically involving the Beighton Screening. Your provider may also discuss or observe any skin-related findings such as atrophic scarring, increased elasticity, and increased stretch marks which are often associated with hEDS specifically. It’s important to also rule out other conditions that may share similar signs and symptoms to HSD, as management of such may differ.
“If you can’t connect the issues,
think connective tissues”-Dr. Heidi Collins
HSD and hEDS are considered diagnoses of exclusion, meaning it can only be diagnosed provided other conditions do not explain the signs and symptoms experienced. Lab tests and imaging do not contribute to the diagnosis of HSD.
Note that a diagnosis can change over time, especially when other signs & symptoms connect more specifically to diagnostic criteria for EDS, or as research is updated. Given the complex and often multi-system nature of HSD, a common phrase has arisen, “If you can’t connect the issues, think connective tissues” (Dr. Heidi Collins).
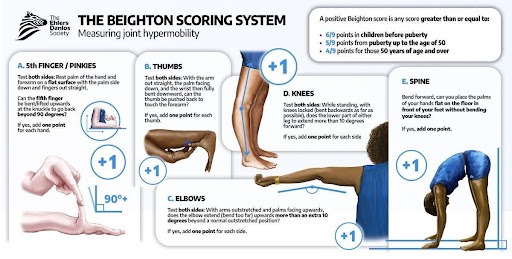 The Ehlers Danlos Society. Beighton Scoring System. Ehlers-Danlos.com
The Ehlers Danlos Society. Beighton Scoring System. Ehlers-Danlos.com
Conditions we attempt to rule out:
- Specific EDS subtypes
- Marfan Syndrome
- Osteogenesis Imperfecta
- Loeys-Dietz Syndrome
- Stickler Syndrome
- Skeletal Dysplasias
- Lupus
- Rheumatoid Arthritis
- Fragile X Syndrome
- Kabuki Syndrome
- Down Syndrome
- Multiple Sclerosis
- Myopathies of various types
Common Co-Occurring Conditions & Overlapping Symptoms of HSD and hEDS
Hypermobility Spectrum Disorder (HSD) and Hypermobile Ehlers-Danlos Syndrome (hEDS) symptoms overlap with a number of other conditions. There are also conditions which may co-occur alongside HSD or hEDS.
HSD & hEDS signs and symptoms may include the following:
- Joint subluxations (partial dislocations)
- Full dislocations
- Acute joint pain
- Chronic or recurrent regional joint pain
- Degeneration and potentially osteoarthritis
- Local sprains or strains to tendons, muscles, ligaments, and cartilage
- Headaches
- Fatigue
- Poor proprioception (awareness of the body’s position in space)
- Gastrointestinal upset-bloating, IBS, incontinence, hernias, food intolerance, etc
- Muscle pain (local or referred)
- Muscle weakness
- Mental and emotional distress
- Disc herniations
- Spinal instability
- Small fiber neuropathy
- Tethered cord
- Rashes
- Easy bruising
- Flushing
- Nerve pain (local or referred)
- Bone pain
Autonomic dysfunction / dysautonomia is a condition where the autonomic nervous system fails to regulate bodily functions like heart rate, digestion, temperature, and blood pressure. It is also associated with HSD and hEDS. Specific symptoms can include dizziness, heart palpitations, brain fog, and chronic fatigue.
Common comorbid dysautonomic conditions:
- Postural Orthostatic Tachycardia Syndrome (POTS)
- Neurocardiogenic Syncope
- Orthostatic Intolerance (OI)
- Vasovagal syncope
Neurodivergence is also linked to joint hypermobility, specifically Attention Deficit Hyperactivity Disorder (ADHD), Autism Spectrum Disorder (ASD), and Tourette Syndrome. The mechanisms through which these conditions are linked are not fully known, however awareness of this association may improve management of HSD and hEDS.
Mast Cell Activation Syndrome (MCAS) may also be associated with HSD & hEDS, however the exact nature of this link is not yet known. MCAS is an immunological condition where mast cells (part of our innate immunity) wrongfully release chemical mediators which cause chronic inflammation and immune symptoms. Some clinical manifestations of MCAS are flushing, fatigue, swollen or watery eyes, anaphylaxis, bloating, rashes, itching, wheezing, and IBS.
Common Treatments & Considerations
A holistic approach is often associated with improved outcomes when it comes to the management of HSD and hEDS. Providers do not necessarily need a formal diagnosis in order to help treat symptoms of these conditions. Treatments for HSD and hEDS are not curative, but instead help the patient manage symptoms, improve overall functioning, and avoid potential complications as best as possible. Surgical options may be necessary depending on the acuity of the condition and overall treatment progression.
Because there is a connection between HSD, hEDS, and metabolic abnormalities proper nutrition and supplementation is suggested to help manage symptoms associated with such. Providers may prescribe certain supplements or encourage diets high in Vitamin D, Vitamin C, Magnesium Bisglycinate, Quercetin, Methylated Folate, electrolytes, Vitamin B6 & B12, Betaine Anhydrous, and Choline among others. Oftentimes individuals will have “safe foods” they prioritize consuming that do not cause as much GI upset or sensory challenges as well.
Massage of various types may also help manage muscle hypertonicity and tenderness in addition to breaking up fascial adhesions that contribute to improper movement and pain levels. In HSD and hEDS, muscles often have to work double time to further stabilize hypermobile joints. Sometimes massage techniques which lengthen muscles too intensely may cause increased instability in a joint, increased pain levels from changes in stability, and in some cases the muscle may spasm shortly after massage. For individuals who find this is the case, I encourage using Trigger Point Therapy, Muscle Energy Techniques (METs), and Myofascial Release as methods of massage.
Chiropractic adjustments are shown to improve pain levels, increase proprioception, and improve joint motion. Providers may opt for low force techniques, adjusting tools (such as an Activator), graded mobilizations, and light traction instead of high velocity low amplitude adjustments (HVLA) to avoid worsening the instability of a joint.
Acupuncture may also assist with decreasing levels of pain, improving proprioception, addressing muscle hypertonicity, as well as managing other symptoms associated with HSD and hEDS such as anxiety, GI upset, and reducing inflammation. Although different from Acupuncture, dry needling is thought to be helpful in managing muscle hypertonicity and pain levels as well.
Individualized physical rehabilitation exercises are a vital component of HSD and hEDS treatment. The goal of rehabilitative exercise in this case is to improve balance, bone density, muscle strength, proprioception, and overall stability of joints. Everyone’s needs and abilities are different, and an exercise that works for one person may not work for another. Providers should be able to meet the patient where they are at, even if that means starting with simple breathing exercises.
General suggestions for rehabilitative exercise:
- Choose an exercise or activity that is fun and engaging for you
- Depending on the level of acuity- you may wish to choose low impact, postural exercises which prioritize lower loads in a small-to-medium
- range of motion. This may include isometrics, balance exercises, use of resistance bands, water aerobics, etc.
- Start slow and pace yourself
- Understand different pain experiences. For instance, you may wish to push through aching pain and muscle soreness during exercise, but not sharp/shooting acute pain that changes your alignment.
- Depending on the level of acuity-avoid high load, high impact, open chain, and large/end range of motion exercises as these may increase pain levels and potential for subluxations.
- Avoid prolonged deep stretching as this may increase instability and joint laxity.
- Understand that some days may be worse than others in terms of fatigue or participation in exercises, avoid shaming yourself.
- Try to choose comfortable settings, perhaps avoid ableist spaces that aren’t body positive or weight inclusive.
People may also wish to use oral or topical analgesics (prescription or OTC) to help manage pain levels.
Compression garments are thought to improve balance and proprioception, especially when combined with physiotherapy. Because of the tendency for arch collapse and instability of the foot and ankle it’s suggested that supportive shoes be worn to reduce potential for sprains, plantar fasciitis, misalignment of knees and hips, or hip impingement. Generally, proprioceptive and dynamic braces are better for allowing activation of muscles and preventing
hyperextension. Whereas static or immobilizing braces are more for acute injuries and may contribute to muscle atrophy over time. Taping can also help stabilize joints in addition to improving proprioception and posture.
Final Thoughts
Overall HSD and hEDS are complex conditions and no two people have the same type or severity of symptoms, nor the same experiences which impact their livelihood or functioning. In this way, the zebra is a fitting symbol representing those with HSD or hEDS, as no two zebras have the same stripes. Physicians are taught the maxim, “When you hear hoofbeats, think horses, not zebras” encouraging them to prioritize common diagnoses (horses) rather than rare ones (zebras). However, as more research is published about HSD and hEDS, we find that this sentiment isn’t always the case. Beyond research arenas, much comfort and understanding of these conditions come from fellow community members with lived experience. Those with HSD and hEDS (as well as caregivers) have built a robust community for guidance, support, and strength on the journey of managing one’s life as it relates to these conditions. Perhaps it’s also fitting that a group of zebras is known as a “dazzle”, because together we can do just that!
“Together We Dazzle!”
-The Ehlers-Danlos Society
Additional Resources
- Disjointed. Navigating the Diagnosis and Management of Hypermobile Ehlers-Danlos Syndrome and Hypermobility Spectrum Disorders. By Diana Jovin and other specialists.
- Holding It All Together When You’re Hypermobile: Achieve a Better Life Experience with EDS, POTS, and Joint Instability. By Christie Cox
- Hacking Hypermobility Podcast by Two Bendy Mommas
- Joint Hypermobility Handbook: A Guide for the Issues & Management of Ehlers-Danlos Syndrome Hypermobility Type & the Hypermobility Syndrome. By Brad T Tinkle
- Taming the Zebra. It’s Much More Than Hypermobility. The Definitive Physical Therapy Guide to Managing HSD/EDS. Volume 1: Systemic Involvement. By Patricia J. Stott and Heather Purdin.
- https://www.facebook.com/groups/oreds
- Oh TWIST-Shining Light on a Twisted Condition. Oh! That’s Why I’m So Tired!
- TikTok @ CirquePhysio Dr. Jen Crane PT, DPT, OCS, ATC “Non-traditional Physio for non-traditional athletes”.
References
- https://www.ehlers-danlos.com/what-is-hsd/#1668010829361-a7fb00ef-40b9
- https://www.ehlers-danlos.com/types/
- Aziz Q, Harris L, Goodman B …AGA Clinical Practice Update on GI Manifestations and Autonomic or Immune Dysfunction in Hypermobile Ehlers-Danlos Syndrome: Expert ReviewClinical Gastroenterology and Hepatology, 2025; 23, 1291-1302.
- Zabriskie HA. Rationale and Feasibility of Resistance Training in hEDS/HSD: A Narrative Review. J Funct Morphol Kinesiol. 2022 Aug 20;7(3):61. doi: 10.3390/jfmk7030061. PMID: 35997377; PMCID: PMC9397026.
- Scheper M, Rombaut L, de Vries J, De Wandele I, van der Esch M, Visser B, Malfait F, Calders P, Engelbert R. The association between muscle strength and activity limitations in patients with the hypermobility type of Ehlers-Danlos syndrome: the impact of proprioception. Disabil Rehabil. 2017 Jul;39(14):1391-1397. doi: 10.1080/09638288.2016.1196396. Epub 2016 Jun 24. PMID: 27339264.
- Csecs JLL, Iodice V, Rae CL, Brooke A, Simmons R, Quadt L, Savage GK, Dowell NG, Prowse F, Themelis K, Mathias CJ, Critchley HD, Eccles JA. Joint Hypermobility Links Neurodivergence to Dysautonomia and Pain. Front Psychiatry. 2022 Feb 2;12:786916. doi: 10.3389/fpsyt.2021.786916. PMID: 35185636; PMCID: PMC8847158.
- Benistan K, Foy M, Gillas F, Genet F, Kane M, Barbot F, Vaugier I, Bonnyaud C, Gader N. Effects of compression garments on balance in hypermobile Ehlers-Danlos syndrome: a randomized controlled trial. Disabil Rehabil. 2024 May;46(9):1841-1850. doi: 10.1080/09638288.2023.2209742. Epub 2023 May 17. PMID: 37194618.
- Benistan K, Foy M, Gillas F, Genet F, Kane M, Barbot F, Vaugier I, Bonnyaud C, Gader N. Effects of compression garments on balance in hypermobile Ehlers-Danlos syndrome: a randomized controlled trial. Disabil Rehabil. 2024 May;46(9):1841-1850. doi: 10.1080/09638288.2023.2209742. Epub 2023 May 17. PMID: 37194618.
- https://gptoolkit.ehlers-danlos.org/
- Smith, Claire. Understanding Hypermobile Ehlers-Danlos Syndrome and Hypermobility Spectrum Disorder. 2024.
- https://hypermobilityclinic.org/hypermobility-tool-kit-tips/
- Russek, Leslie and De Wandele, Inge. 07/30/2019-08/01/2019. Physical Therapy Management. Youtube. https://www.youtube.com/watch?v=wBBLIbe2dvM
About The Author
 Dr. Brandy “B” Hagan is a Chiropractor in Portland, OR who focuses on treating individuals with Hypermobile Spectrum Disorder and Hypermobile Ehlers-Danlos Syndrome. Their lived experience with HSD drives much of their treatment approach and considerations when working alongside patients with similar conditions.
Dr. Brandy “B” Hagan is a Chiropractor in Portland, OR who focuses on treating individuals with Hypermobile Spectrum Disorder and Hypermobile Ehlers-Danlos Syndrome. Their lived experience with HSD drives much of their treatment approach and considerations when working alongside patients with similar conditions.